For healthtech founders and product teams evaluating AI integration strategies for healthcare: what works, what fails, and where to start without wasting runway.

Highlights
- Most healthcare AI pilots never reach production due to poor data readiness, not the technology.
- Physicians average 27 hours of direct patient care weekly; documentation consumes the rest.
- A 2025 JAMA study found AI scribes saved 16 minutes of documentation per clinical shift.
You have a live healthcare product, and you're evaluating whether AI integration makes sense for your specific situation. And if so, where to start?
Technology is rarely the obstacle.
What kills healthcare AI projects is scoping gaps, data that wasn't audit-ready, compliance requirements that surface three months into development, and models that get deployed but never used because no one designed for the clinical workflow they were supposed to fit into. By then, the timeline has doubled, the scope has been cut, and the clinical team has already found a workaround.
This article covers what to build, in what order, and what to get right before writing a line of code.
Mind Studios has built HIPAA-compliant, AI-integrated products across diagnostic support, remote monitoring, and clinical workflow tooling. We offer a free technical consultation before any contract is signed. Contact us to get an honest read on what is realistic for your product.
Benefits of integrating AI into healthcare software
Most teams start by asking what AI can do, but the more useful question is what it fixes that your current stack cannot.
The impact of AI on healthcare products is most visible in five areas.
| Benefit | What it means in practice | Best for | How it's built |
|---|---|---|---|
| Faster clinical decision support | Reduces time from data collection to diagnosis recommendation. | Diagnostic platforms, EHR-integrated tools. | ML models on structured patient data. |
| Reduced administrative load | Automates intake, documentation, coding, freeing clinical staff for patient care. | Practice management platforms, hospital ops tools. | NLP, RPA, ambient scribing. |
| Personalized care at scale | Enables adaptive care plans based on real patient data without manual intervention. | Chronic disease apps, remote monitoring platforms. | Predictive analytics, recommendation engines. |
| Earlier risk detection | Flags patient deterioration or disease markers before they become critical events | Remote monitoring, wearable-integrated platforms, population health tools. | Anomaly detection, time-series ML on wearable data streams. |
| Accelerated product differentiation | Adds capabilities that commodity EHRs cannot replicate, creating a competitive moat. | Health startups competing with off-the-shelf platforms. | Custom model training, specialty-specific algorithms. |
Healthcare AI is not a feature you ship, but a system you grow. The teams that treat it as a one-time build consistently run into the same problems six months after launch. The ones that plan for ongoing refinement from day one are the ones that see real outcomes.
— Dmytro Dobrytskyi, CEO at Mind Studios.
Not sure which of these applies to your product? Talk to our team, and we will review your setup and tell you honestly what is realistic.
Let’s explore tech
solutions
Get our expertise

Mind Studios’ insight: The most common mistake we see at the integration stage is treating AI as a feature to bolt on rather than a workflow to redesign around. A model that improves diagnostic accuracy but sits outside the clinical workflow your team already uses will not get adopted. And without adoption, there is no data, and without data, the model cannot improve. Build for the workflow first, then the model.
The question then becomes: which workflows are realistic candidates for AI integration in your specific product?
Where AI earns its place in a healthcare product
Not every AI application in healthcare is relevant to a product team with a live system and a real deployment timeline.
The three categories below cover where AI in healthcare software integration decisions are actually being made: in clinical workflows, patient-facing products, and operational systems.
Each one has a different entry point, different regulatory implications, and a different timeline to measurable impact.
Diagnostic and imaging products
When a platform surfaces imaging data, the architecture decision that matters most is not which model to use. It is whether the product displays clinical data or helps interpret it.
A display layer shows the image. A decision-support layer flags anomalies, prioritizes worklists, and surfaces comparison data that shapes a clinical decision. Those two products have different scopes, different validation requirements, and different regulatory obligations.
A product that influences clinical decisions based on imaging falls under the FDA SaMD classification. The compliance path needs to be scoped before development starts, not added once the product is built.
AI technologies commonly used in diagnostic and imaging products:
- Machine learning for identifying relationships between clinical data, symptoms, and disease outcomes.
- Deep learning applied to medical images, including X-rays, CT scans, and MRIs.
- NLP for interpreting clinical notes and unstructured medical records.
- Decision support systems drawing on patient history, symptoms, and real-time test results.
- Probabilistic reasoning for assessing the likelihood of various diagnoses.
Patient-facing products
AI in patient-facing products covers three distinct integration points: each with different technical requirements, different regulatory implications, and a different relationship to the clinical workflow. The right starting point depends on where your product sits in the care journey.
Ambient documentation
Ambient scribing market reached $600M in 2025, growing 2.4x year over year. Tools that passively capture clinician-patient conversations and generate structured notes integrate directly into EHR systems, saving measurable documentation time per shift.
No custom model training required, and no rearchitecting of existing EHR workflows, which is why adoption has moved faster here than in any other clinical AI category.
Wearable-integrated platforms
Continuous data streams (such as heart rate, movement, and sleep) generate more signals than any clinical team can manually review. AI models trained on these streams detect early markers of arrhythmia, cardiovascular risk, and chronic condition deterioration before a patient reports symptoms.
Two decisions that consistently get underestimated at the build stage:
- EHR integration. Integrating AI with EHR software is what makes wearable data clinically useful because a product that collects data but does not push it into the EHR creates a parallel stream clinicians cannot act on. How wearable data is structured, mapped, and written back to the EHR needs to be scoped before development starts, not added later.
- Device classification. Consumer wearables like Apple Watch or Fitbit and medical-grade wearables operate under different regulatory frameworks. Building clinical decision-making on top of consumer wearable data means relying on a source that was not FDA-cleared for that purpose. This is a compliance risk that surfaces late: design the data layer for your actual regulatory context from the start.
Conversational AI
Handles symptom triage, medication reminders, post-discharge follow-up, and patient routing without clinical staff involvement. The build decision comes down to one distinction: rule-based chatbots follow a fixed script and break when a patient phrases something unexpectedly.
NLP-powered models understand intent rather than keywords, which is what real patient communication requires. Both integrate with EHR systems, pulling patient history to personalize responses and pushing interaction data back into the clinical record.
Other common applications in patient care products:
- Medication management tools for reconciliation, adherence monitoring, and personalized recommendations.
- Chronic disease management platforms providing adaptive care plans and symptom monitoring.
- Fall detection solutions using sensors, wearables, or camera-based technologies with anomaly detection.
Operational workflows
Using AI in healthcare software for administrative and operational workflows is often the lowest-friction entry point for a healthcare product, and among the fastest to show measurable ROI. These integrations sit outside direct patient care, which reduces regulatory complexity and shortens the path to deployment.
Common AI applications in healthcare management products:
- Revenue cycle management tools that automate billing, coding, and claims processing, and flag potential revenue leakage.
- Supply chain platforms using historical data to forecast supply needs and automate procurement.
- Fraud detection services analyzing patterns and anomalies in claims data and billing practices.
- EHR workflow automation through RPA covering scheduling, documentation processing, and administrative tasks.
- Predictive staffing platforms optimizing resource allocation based on historical patient data and admission rates.
How healthcare AI integration actually works
AI healthcare solutions integration fails more often at the planning stage than the technical one. The six steps below cover what the process actually looks like when done correctly.
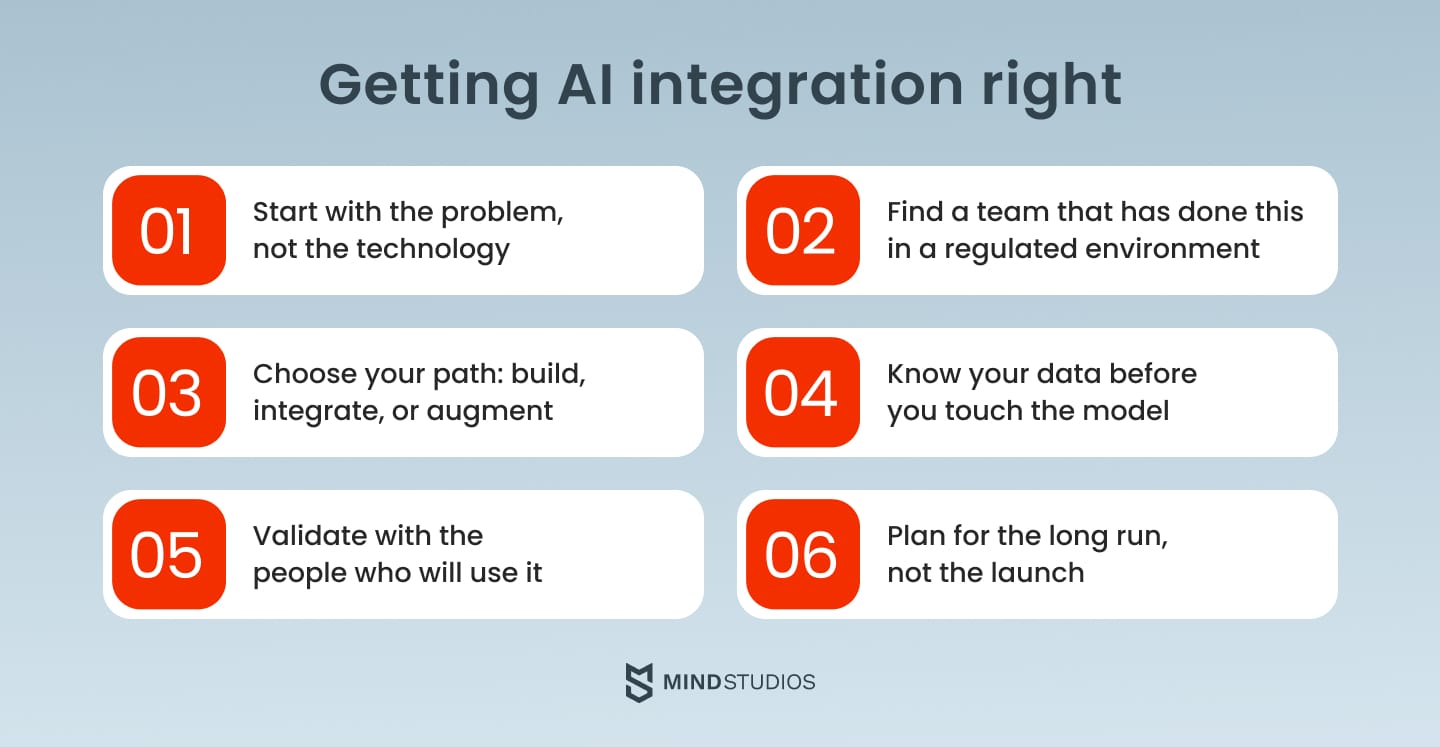
Step 1. Define the problem AI needs to solve
The starting point is not "how do we add AI", it is "what problem in our product cannot be solved without it."
A well-scoped AI project starts with a specific workflow, a specific failure point, and a measurable outcome. Without that clarity, model selection and data preparation have no foundation to build on.
Mind Studios’ insight: A useful test: if the same outcome could be achieved by hiring one more analyst or adding a filter to an existing dashboard, it is not an AI problem. AI earns its place when the data volume, the pattern complexity, or the real-time requirement exceeds what a human or a rule-based system can handle.
Step 2. Choose the right technical partner
AI in healthcare software development requires a team that combines AI capability with healthcare data architecture experience and compliance familiarity.
Most teams have one or two of those, not all three. During evaluation, ask specifically about HIPAA and GDPR experience, post-launch availability, and how they have handled regulatory complexity in previous healthcare projects.
What separates teams that succeed here from those that stall is not technical capability alone. A team that has built HIPAA-compliant AI-integrated products before knows where the risks are and how to design around them from the start. A team encountering those constraints for the first time discovers them mid-project.
Mind Studios’ insight: Integrating with systems like Epic requires specialists who have done it before. The architecture decisions that determine whether that integration holds up are made before development starts, not during it.
One example is Dr. CHO, a pre-visit medical platform we built that uses intelligent algorithms to adapt clinical intake questions based on patient responses. It is fully integrated with existing EHR workflows and built to HIPAA compliance standards from day one.
Want to know if Mind Studios is the right fit for your integration? Book a free consultation before any contract is signed.
Let’s discuss
your tech
needs
Contact Mind Studios
Step 3. Decide between build, integrate, or augment
Three paths exist when you integrate AI solutions in healthcare products, and the right one depends on your product, your data, and your timeline.
- Building a custom AI model from scratch gives maximum control but requires clean training data, clinical validation, and significant development time.
- Integrating a ready-made solution is faster but creates dependency on a third-party model that was not trained on your specific data.
- Augmentation is how most successful healthcare AI products are being built right now. Rather than replacing existing systems, an AI layer connects to them and automates a specific workflow: documentation, prior authorization, and risk flagging. It is faster than custom development, less dependency-creating than off-the-shelf models, and works within the EHR infrastructure clinical users already trust.
Your technical partner should help you evaluate which path fits your product before you commit to any of them.
Whichever path you choose, the next constraint is the same: your data.
Step 4. Audit your data before writing a line of code
Data readiness is the most common failure point in healthcare AI projects. Teams assume their EHR data is clean and structured. It almost never is. Patient records contain inconsistent formatting, missing fields, and labeling gaps that only surface once model training begins at which point the timeline has already been set.
A proper data audit before development starts covers what data exists, what format it is in, what is missing, and what preparation work is required before it can train a model. That audit should happen before the scope is finalized, not after.
The failure mode in healthcare AI is almost never the technology. It is the assumption that the project can succeed without quality data and clinical validation in place before development starts. Teams that skip the data audit to move faster consistently spend more time recovering from it than the audit would have taken.
Mind Studios’ insight: In our experience, data preparation consistently takes longer than teams expect, and the gap between "we have the data" and "the data is ready to train on" is where most AI timelines slip.
Step 5. Validate with the people who will actually use it
Implementing AI models into healthcare products begins once data is prepared — training and testing can start only when the data audit is complete. Engineers validate that the model performs against technical benchmarks.
But clinical validation is a separate step, and not optional. The clinicians who will use the product in practice are the ones who confirm whether it performs against clinical reality, catches what it should catch, and behaves reliably across the patient populations it will encounter.
Involving clinicians before the build, not after, is what makes the difference. Their input at the design stage shapes workflow fit, interface decisions, and edge case handling in ways that no amount of post-launch iteration can fully recover. A model validated only by engineers is not a validated model.
Step 6. Plan for what happens after launch
Deployment is not the end of the project. Healthcare AI systems require continuous monitoring, user feedback loops, and ongoing model refinement. Clinical environments change, patient populations shift, and edge cases that did not appear during testing surface in production.
AI projects in healthcare are not delivered, they are grown. At Mind Studios, 70% of clients continue using our maintenance and support services three or more years after project launch.
We worked with the Envol team through their initial launch, a full user migration, a fundraising round, and ongoing feature development. That is what long-term looks like in practice, and it is the difference between a vendor that hands off and a partner that stays.
Why healthcare AI projects fail before they ship
AI integration in healthcare is not technically harder than in other industries. What makes AI and healthcare software different from other integration contexts is the consequences of getting it wrong.
The challenges below are not edge cases but the failure points that appear consistently across healthcare AI projects, regardless of team size or budget.
Compliance built in too late
Medical data is among the most regulated in any industry.
HIPAA in the US, GDPR in Europe, and equivalent frameworks elsewhere set strict requirements for how patient data is collected, stored, processed, and shared.
AI systems that require access to large volumes of patient data to function create real exposure if those requirements are not built into the architecture from the start.
Compliance is not a final checklist before launch. It is a design constraint that shapes how data is structured, how access is controlled, and how the audit trail is maintained throughout the system. Teams that treat it as an afterthought consistently hit compliance-driven delays that push timelines back months.
Models trained on the wrong data
AI models reduce certain categories of human error, but they introduce others.
A model trained on incomplete or unrepresentative data will produce outputs that reflect those gaps, sometimes in ways that are difficult to detect without clinical expertise.
In healthcare, where a missed diagnosis or a false positive carries real consequences, the quality of training data and the rigor of clinical validation are not optional considerations.
The standard that matters here is not whether the model performs well on a benchmark dataset. It is whether it performs reliably across the actual patient population it will encounter in production.
Tools clinicians work around instead of with
A tool clinicians do not use generates no data. A tool that generates no data cannot improve.
Adoption resistance in clinical settings is rarely about the technology itself but about workflow disruption, unfamiliar interfaces, and the perception that a new system adds steps rather than removes them.
Building for adoption means involving clinicians in the design process before the product is built, not after. Their input on workflow fit, interface design, and edge cases is what separates a tool that gets used from one that gets bypassed.
Shadow AI
By the time a clinical AI feature reaches a product roadmap, clinical staff have often already started solving the same problem with consumer tools:
- ChatGPT for discharge summaries.
- Voice memos transcribed by consumer apps.
- Screenshots sent to a chatbot.
None of it is HIPAA-compliant. None of it appears in an audit trail.
Before building an AI feature, check whether your users have already solved the problem themselves, and how.
Designing against an existing informal workflow is significantly harder than designing for one that does not exist yet. A structured discovery process before development starts is what surfaces this. It is one of the reasons we run a business analysis phase before writing a line of code.
Avoiding these failure points starts before development begins. If you want an honest read on where your product stands, we offer a free technical assessment.
The regulatory landscape your product is building into
Compliance gaps surface late because regulatory requirements are misunderstood early. Here is the current status across the three regions most relevant to healthtech products.
United States
There is no comprehensive federal AI legislation specific to AI integration for healthcare. AI in clinical settings is governed by existing frameworks: HIPAA covers patient data privacy and security, and the FDA regulates AI-powered software that meets the definition of a medical device under its SaMD guidance.
If your product influences a clinical decision, confirm whether it falls under FDA oversight before development begins. Several states have also introduced their own AI-related requirements that may apply depending on where your product operates.
European Union
The EU AI Act entered into force in August 2024 and is now law across all member states. For healthtech products, the key provisions cover high-risk AI systems: clinical decision support tools, diagnostic software, and AI that influences treatment decisions.
High-risk systems require conformity assessments, documented risk management processes, and ongoing post-market monitoring. GDPR continues to apply in parallel. If your product operates in the EU or processes data from EU patients, both frameworks apply simultaneously.
United Kingdom
The UK has not introduced AI-specific legislation, though the government has signaled a pro-innovation stance. AI in healthcare currently falls under UK GDPR, the Data Protection Act 2018, and MHRA medical device regulations. The framework is less prescriptive than the EU's but is developing — products entering the UK market should monitor MHRA guidance actively.
We have built HIPAA-compliant products and can help you identify which regulatory requirements apply to your specific product before development begins. That conversation is part of our free technical consultation. Just contact us.
Conclusion
Integrating AI into healthcare software is not a project with a finish line.
The teams that treat it as a feature launch (scope it, build it, ship it, and move on) are the ones who end up with models that degrade, workflows that get bypassed, and compliance gaps that surface at the worst moment.
The products that work are built on clean data, designed around clinical workflows, and supported by a team that stays involved after launch.
If you are evaluating AI integration for a healthcare product, we are happy to look at your current setup and give you an honest assessment. That is how we start every engagement. Contact us.